






































- The study of disease transmission:
Bladder Cancer (BC) is the most notable risk of the urinary lot and the seventh most ordinary threatening development in men and the seventeenth in women. Event shifts among regions and countries. The world overall age-standardized demise rate is 3 for men versus 1 for each 100,000 for women. The pace of BC has decreased in specific vaults possibly reflecting a reduced impact of causative trained professionals, basically smoking and word-related show
The mortality of BC has moreover been reduced possibly reflecting the extended norm of care
Generally, 75% of patients with BC present with the contamination that is kept to the mucosa (Stage Ta, CIS) or submucosa (Stage 1). These classes are accumulated as non-muscle-prominent bladder-threatening development (NMIBC). Non-muscle meddling BC has a high inescapability due to low development rates and long stretch perseverance all around. Patients with muscle-meddling bladder dangerous development (MIBC) are at higher risk of illness unequivocal mortality. The ordinariness of BC is among the most raised of all urological malignancies.
2. Hazard Factors:
Extending verification suggests that inherited tendency influences bladder threat events especially through its impact on shortcoming to other peril factors. Tobacco smoking is the main peril factor for BC, addressing? a big part of the cases (3, 7). Tobacco smoke contains sweet-smelling amines and polycyclic sweet-smelling hydrocarbons, which are really released. Word-related prologue to fragrant amines, polycyclic sweet-smelling hydrocarbons, and chlorinated hydrocarbons is the second most critical risk factor for BC, accounting in the high-level time? 10% of things being what they are. Such word-related presentation happens mostly in current branches dealing with paints, shading, metal, and oil-based items (3, 8-10).
The association between the singular hair shading use and BC peril stays sketchy; extended risk has been proposed in customers of enduring hair tones with NAT2 moderate acetylation aggregate.
The course of action:
A papillary Bladder cancer restricted to the within layer (Mucosa) is assigned stage (Ta) as shown by the Tumor, Node, Metastasis (TNM) portrayal structure. Cancers that have assaulted the internal layer (lamina propia) when assigned Stage T1. Ta and T1 growths can be emptied by transurethral resection (TUR), and thusly they are gathered under the heading of Non-Muscle-Invasive Bladder Cancer (NMIBC) for helpful purposes. Similarly included under this heading are level, high-grade cancers that are confined to within layer (mucosa), and named CIS (Tis). In any case, nuclear science strategies and clinical experience have shown the significantly undermining capacity of CIS and T1 injuries. Thusly, the terms NMIBC and shallow BC are defective depictions.
The cancer stage and grade should be used for medicinal purposes.
The histological investigating of all bladder urothelial carcinomas were proposed and dispersed by the WHO in 2004 (15, 16), this request consolidates the level of bruises as urothelial hyperplasia, responsive urothelial atypia, dysplasia, and CIS. Among Non-Invasive papillary urothelial wounds, 2004 WHO checking on isolates between papillary urothelial neoplasm of low destructive potential (PUNLMP) and low quality and high-grade urothelial carcinomas.
Papillary urothelial neoplasm of low hazardous potential (PUNLMP) is portrayed as bruises that don’t have cytological features of danger yet show commonplace urothelial cells in the papillary arrangement. Despite the way that they have a superfluous peril for development, they are not absolutely ideal and still will in general rehash. 3) Diagnosis:
A. Lenient history should be taken and recorded for astoundingly huge information with a possible relationship with Bladder Tumor; including peril components and history of suspect incidental effects.
B. Signs: Hematuria is the most notable finding in NMIBC. Ta, T1 cancers don’t cause bladder torture, and sometimes present with lower lot signs (LUTS). In patients who do complain of these signs particularly in those with irritative LUTS willful to intriguing treatment, CIS might be suspected.
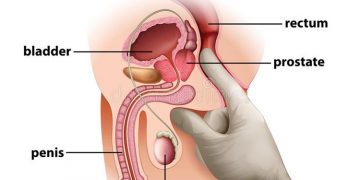
C. Actual Examination: the actual appraisal doesn’t uncover NMIBC anyway tremendous urothelial cancer assaults the bladder divider and different organs.
D. Imaging:
an) Intravenous Urography (IVU): Large exophytic growths maybe saw as a filling gives up in the bladder
b) Computed Tomography (CT): This assessment gives a bigger number of information than IVU does (counting status of lymph centers and adjoining organs)
c) Ultrasonography (US): The US is much of the time used as the hidden device to assess the urinary lot. The transabdominal US awards depiction of renal mass, area of hydronephrosis, and portrayal of intraluminal masses in the bladder. It will in general be pretty much as exact as IVU for the assurance of the upper urinary parcel obstruction (17).
The US is consequently an accommodating device for the area of obstructions in patients with haematuria, in any case, it can’t dismiss the closeness of upper plot growths.
CIS is not set in stone to have imaging methods (IVU, CT pyrography, or the US).
d) Urinary Cytology: Examination of voided pee or bladder-washing models for stripped cells has high affectability in below-average cancers. In light of the loss of cell connection in the epithelial covering of the bladder in CIS, there is a greater number of floating cells in the pee, similarly to a genuine degree of anaplasia. The affectability of cytology for CIS area in 28-100%.
Cytology is accordingly useful when high-grade damage or CIS is accessible. Positive voided urinary cytology can show urothelial cancer wherever in the urinary lot, from the calyx to the ureters, bladder, and proximal urethra.
Negative cytology, in any case, doesn’t bar the closeness of cancer in the urinary parcel.
e) Urinary nuclear marker test: Driven by the low affectability of pee cytology, wide lab research has developed different urinary tests for the BC area (19-25).
Considering the repeat of cystoscopy for advancement, markers for the discontinuous urothelial infection would be especially significant.
Microsatellite examination is the most uplifting of the methods recorded in the Table under (26-28).
g) Transurethral resection of Ta, T1 bladder cancers: The goal of the TURB in Ta, T1 BC is to make the right assurance and clear each and every recognizable injury.
It is a huge framework in the finding and treatment of BC.
The methodology of resection depends upon the size of the injury. Little cancers









{kind=link}
Discussion about this post